The following information is for patients who are experiencing lateral hip pain which has been diagnosed as coming from the gluteal tendons. It covers what gluteal tendinopathy is, why it happens, what the symptoms are, pain onset and how it is diagnosed and treated. It offers advice on how a patient can help themselves, including positions that will reduce aggravation of the tendons, and static and dynamic stage 1 exercises that will help to reduce pain and aid with strengthening.
Traditionally, pain over the lateral hip (pain on the side of the hip and thigh) has always been referred to as ‘trochanteric bursitis’ (bursitis is inflammation of a fluid-filled sack which protects the tendon from bone). We now know that issues with the bursa are rare in isolation, and it is an inconsistent feature of lateral hip pain (isolated bursitis is rare, shown in only 2% of patients). Research has shown that issues with the tendons co-exist with issues with the bursa and it usually co-presents with tendon pathology (88 to 98% of patients have tendon pathology). However, the most recent evidence shows that the primary cause of lateral hip pain is due to pain from the tendons of gluteus medius or minimus that attach the muscle to the bone. These tendons are from the gluteal muscles (buttock muscles) that arise from the pelvis and attach to the greater trochanter, the bony point at the side of the hip. Therefore, it is now known as ‘greater trochanteric pain syndrome’ (GTPS) and ‘gluteal tendinopathy.’
Gluteal tendinopathy is the most common tendinopathy affecting the lower limbs. It is more common in females than in males (4x as many women get GTPS than men) and can affect up to 25% of adults. The condition is most common in peri- and post-menopausal females, present in 23.5% of women and 8.5% of men between the ages of 50 and 79. Pain in the lateral hip has been reported in up to 77% of patients with hip osteoarthritis. This condition can also occur in the young athletic population and is particularly an issue with runners or those involved with step training.


Why does gluteal tendinopathy happen?
The exact causes of gluteal tendinopathy are still being explored, but it is often associated with weakening of the gluteal muscles and movements that increase the stress on the gluteal tendons. Compression of the gluteal tendons over the greater trochanter is thought to be a key factor in the development of gluteal tendinopathy and can be linked to certain postural habits and movement patterns, such as hip hanging or excessive movement of the hip inwards on loading. There are, however, a multitude of other contributing factors for developing gluteal tendinopathy, including:
- increased weight around stomach
- diabetes
- genetic factors
- previous use of Fluoroquinolone antibiotics
- high cholesterol
- hormone changes
- vascular issues
- age
- spinal/hip pathology
Any of these factors can make you more susceptible to developing gluteal tendinopathy; often, it is a combination of factors.
In younger populations, it often occurs in runners or those people participating in activities involving step-up or lunging tasks. Gluteus medius and minimus (two of the hip muscles) tendinopathy may co-exist with hip joint pathology. Degenerative tears of these tendons have been seen in 20% of patients with osteoarthritis. It also occurs in 20 to 35% of patients with lower back pain.
There is also suggestion in the research of a link between bony structure of both the femoral neck and the acetabulum (socket), the forces imposed on the soft tissues and the development of pathology, but further research is required.
The symptoms
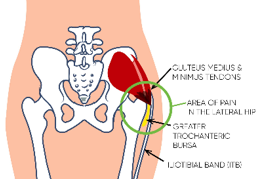
The most recognised feature of gluteal tendinopathy is pain and tenderness on the outside of the hip directly over the greater trochanter (the bone at the side of the hip). Pain can also extend down the lateral thigh to the knee and may radiate anteriorly or posteriorly to the greater trochanter. Pain is often felt as sharp pain over the greater trochanter on compression or may be aching or burning in nature. Sharp pain may also be associated with snapping or clicking and this can occur when the iliotibial band (band of connective tissue at the side of your leg) crosses over the greater trochanter. Patients can also report feelings of ‘giving way’ during weight-bearing tasks. Pain can be felt:
- when lying (on either side)
- on single leg loading (such as standing on one leg to get dressed)
- on sitting for a prolonged period in low chairs or car
- on rising from a chair for first few steps
- on walking up hills or stairs
- on running
- when touching on the lateral hip bone
Pain onset
Gluteal tendinopathy often becomes symptomatic when a tendon that is weak is exposed to a sudden increase in loading, for example hill walking or walking a much longer distance than normal or climbing lots of stairs. Tendons can react when a change of load has occurred, such as too much or too little loading, for example after a period of rest.
It can also occur after a direct impact to the greater trochanter, such as a slip or fall which resulted in landing onto the greater trochanter and therefore a sudden increase in load and compression on those tendons. However, it is multifactorial and often it is difficult to identify a specific incident, and it can therefore be due to a gradual deterioration in tendon health over time, alongside load changes and compression elements. Subsequently, the overload on the tendon becomes too much, and tendon pain occurs.
Thus there is a continuous cycle:
- increased pain, leading to
- tendon irritation due to overload/compression from day-to-day activities, leading to
- muscle fatigue and tightness, leading to
- pain and reduced hip range of movement, leading to
- too much rest and lack of use can cause muscle weakness, leading to
- increased pain... and so on.
How gluteal tendinopathy is diagnosed
In most cases your doctor or physiotherapist will suspect gluteal tendinopathy from the symptoms you describe and from a cluster of tests they will complete when they physically examine your hip. These can include palpation of the side of your hip, single leg balance test, resisted side lying abduction test, a hip rotation test and others. Sometimes, further diagnostic tests such as ultrasound or MRI (magnetic resonance imaging) scans are used, but these are not required for confirmation of the diagnosis.
Treatment
A detailed assessment of your hip will be completed by your physiotherapist or medical professional. They will also assess your postural and movement habits, and discuss your day-to-day activity. The best treatment for gluteal tendinopathy, according to the most up-to-date evidence, is physiotherapy.
Treatment should focus on:
- Reduction of compression of the tendons over the greater trochanter.
- An exercise programme which should focus on the correct control, recruitment and capacity of the muscles around the hips and pelvis.
Gluteal tendinopathy is multi-factorial, so your physiotherapist will discuss with you all factors that could be contributing to your pain, such as weight management, diet, hormones, activities etc. You will also be advised on adjustments to work/hobbies/leisure activities that may be required to settle your pain.
What can I do to help myself?
Pay attention to your posture
The quickest way to make a difference is to reduce the compressive load on the tendon by preventing any postures that aggravate the tendon and load the lateral hip – any position where the hip is moved out the side relative to the knee. The following should help:
- do not stand with one hip ‘hung to the side’, such as when holding a child on your hip
- do not bring the knee across the body – don't sit cross-legged
- do not do buttock stretches.
The first step to treating gluteal tendinopathy is to decrease the amount of compression on the tendon, both during the day and at night. Postural activity modifications are vital.
Sitting
- Minimise the time spent crossing your ankles or legs.
- When you sit, aim to sit with the hips higher than the knees, and try not to sit on low chairs. Using a wedge cushion may help to keep the hips higher than the knees.

Sleeping
- If you sleep on your side, try to avoid sleeping on the sore hip. Place a pillow between your knees to keep your hips in neutral alignment.
- Another sleeping position that can be helpful is semi-prone (halfway between lying on your tummy and your side, to avoid direct compression on the affected hip). Again, pillows need to be used to support the top leg and in front of the trunk to avoid rolling fully onto your tummy and the underside hip can be straightened.
- If both hips are painful, an option is to sleep on your back with pillows under your knees.
- An eggshell mattress topper can be helpful, as it reduces the amount of compression through the hips.

Functional movements
Your physiotherapist will assess you and advise on specific movement and postural adaptations to you, but here are some you can try:
- Avoid hill walking and stairs where possible.
- Try not to walk too far in a day and minimise walking distance where able.
- When standing, try to keep your weight distribution equal through both feet and do not hang on one hip.
- When stair climbing, use a rail on the opposite side to the painful hip and try to put your leg a little wider and minimise the rolling inwards of the knee.
- Avoid end range, prolonged stretching of the hip.


Lifestyle changes
- Maintaining a healthy weight is important to reduce the likelihood of further flare-ups.
- Healthy diet as per NHS 'Eatwell plate' is recommended.
- Smoking cessation: smoking has been shown to adversely affect the health of tendons.
- Low cholesterol and low saturated fat diet: high cholesterol affects tendon health and is important to manage to minimise tendon pain.
- Discuss pain relief with pharmacist or GP as required.
- Relaxation and mindfulness.
Should I consider a corticosteroid injection?
- Physiotherapy, compression and load management should be the first port-of call before considering a steroid injection.
- Steroid injections can aid with pain relief in the short term (three to six months) in low- to moderate-grade tendinopathy. Caution should be considered, as steroids can have potential negative effects on tendon health in certain tendons.
Exercises
Changes in abductor muscle size and quality have been shown on MRI studies in those patients with lateral hip pain. Fatty atrophy of the gluteus medius and minimus has been observed; this means that there is a combination of reduced muscle size and the replacement of muscle tissue with fat.
Studies looking at muscle strength in gluteal tendinopathy have demonstrated that if pathology is present in one hip, the gluteal strength of both hips is affected. On average, the symptomatic side is 32% weaker, and the non-symptomatic side is 23% weaker than patients without gluteal tendinopathy. Therefore, it is key to strengthen both hips in the presence of gluteal tendinopathy.
- Avoid any stretching as this will increase compressive forces applied over the greater trochanter and aggravate symptoms. Avoid gluteal stretches, strong lumbar rotation stretches or ITB (Iliotibial band) stretches – see image below.
- Load management: minimise time spent in provocative postures such as sitting cross-legged, hip hanging, and minimise walking distance.
- Avoid hill and stair climbing.
- If doing floor-based Pilates, avoid clams and side lying leg lifts as these both increase compression and friction at the greater trochanter.
- Gait re-training: smaller stride length, leading with the knee and landing softly.
- Graded strengthening programme.

Stage 1 exercises
- The early exercises are designed to start strengthening your muscles without irritating the pain.
- The exercises labelled ‘P’ can help ease pain. Do these every day if you have hip pain, even if you are having a flare-up.
- The exercises labelled ‘S’ are strengthening exercises. Do a selection of these at least four times per week.
- Muscle ache during exercise is OK but it should settle quickly and feel no worse as a result later. If it does, reduce the number you are doing and discuss it with your physiotherapist.
Exercise 1: Static muscle activation (P)
Starting position: Sitting. Knees bent and hip width apart. Feet flat on floor.
Action: Imagine that your feet are resting in a sandpit. Steadily push the soles of your feet out into the sand as though trying to leave a convincing impression in the sand.
Hold time: 10 to 20 seconds. Relax slowly.
Number of repetitions: 4 reps 3 sets

Exercise 2: Static muscle activation (P)
Starting position: Sitting. Knees bent and hip width apart. Heels together. Put a cushion or something soft between your heels if needed for comfort.
Action: Steadily squeeze your heels together.
Hold time: 10 to 20 seconds. Relax slowly.

Exercise 3: Static muscle activation in lying with belt (P)
Starting position: Lying on your back pillow under your knee, hips hip width apart. Belt around the top of the knees (as shown).
Action: Steadily squeeze your knees out into the belt- feeling an activation in your bottom.
Hold time: 30 seconds. Relax slowly.

Exercise 4: Static muscle activation in sitting against belt (P)
Starting position: Sitting. Knees bent and hip width apart. Feet flat on floor. Place a strong leather belt, luggage strap or similar around your lower thighs.
Action: Steadily push your knees out into the restraint, feeling an activation in your buttock. Do this slowly, like turning up the button on the radio.
Hold time: 30 seconds. Relax slowly.
Number of repetitions: 4 reps 3 sets

Strengthening exercises
Exercise 5: Bridge with belt (S)
Starting position: Lying on back, knees hip width apart and bent to roughly 90°. Feet apart on floor/bed. Belt around your knees gently squeeze out into the belt.
Action: Slowly roll your pelvis back and tuck your tail bone in. This flattens your lower back into the floor/bed. Then slowly push through your heels and raise your bottom off the bed.
Hold time: Five seconds. Relax slowly.
Number of repetitions: 8 reps 3 sets
Progression: As above and then place your feet in a step stance position.

Exercise 6: 4-point kneeling core activation (S)
Starting position: Kneel on all fours with your knees and hands hip width apart. Stomach relaxed. Keep your spine straight throughout.
Action: Draw your lower tummy (area below the belly button) in towards your spine. The effort needed to do this should not be more that 50% of the maximum effort you could try. Breathe normally.
Hold time: 10 to 20 seconds. Relax slowly.
Number of repetitions: 4 reps
Progression: As this gets easier, start to add a buttock clench at the same time.

Exercise 7: Sit to stand with belt (S)
Starting position: Sitting. Knees bent and hip width apart. Feet flat on floor. Arms folded across your chest. Belt around your knees squeezing out into the belt.
Action: Tighten your buttocks then slowly stand up maintaining the 'squeeze' of your buttocks. Then do the same to sit down slowly. Keep your feet and knees apart throughout.
Number of repetitions: 8 reps 3 sets
Progression: Start with a high chair; as it gets easier, move to a lower chair.

Key messages
- Hurt doesn’t equal harm: pain is not a direct indication of damage.
- Pain is multifactorial; many things impact pain levels, such as poor sleep, stress, poor diet and high BMI (body mass index), alcohol, smoking and low activity levels.
- Reconditioning your hip and building up tendon strength and capacity is key to all the tasks you need to do.
- Striking a balance between working hard enough to recondition the tendons but respecting their sensitivity is key. Listen to your pain.
- Think of pain like a traffic light system: 0 to 4 is green pain, 4 to 6 is amber pain and 7 to 10 is red pain. Be cautious exercising in amber and do not push into red pain.
Beware of latent tendon pain
Monitoring night-time pain can be useful for how the hip is tolerating loading. If pain increases at night, it can highlight that the activity completed that day or within the last two days may have been too much for the tendon and therefore should be reduced. You can push into a tolerable amount of pain that settles within an hour or so; this means the load is correct.
Prognosis
- Early diagnosis and management of load and compression with physiotherapy can see symptoms change quickly.
- The most optimal outcomes are achieved over a period of at least 12 weeks of exercise.
- Two-thirds of people will see their symptoms resolve within a year.
- Gluteal tendinopathy is a degenerative process with significant implications on quality of life.
- It is important to seek advice on management.
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/